Breaking Down Walls: How We Built a Palliative Care Collaborative
Inspiration: The Story of Our Collaborative
Palliative care is a relatively new health care discipline in the United States. A lack of broad understanding of this developing specialty, in addition to a limited workforce and staffing deficits results in only a handful of providers at most hospitals, and even fewer in outpatient and home settings.
Despite the fact that the Philadelphia area is widely recognized for its excellent health services and many excellent health care systems, health care is silo’d by setting as it is across the nation. Systems compete and do not collaborate. In-patient settings work in near complete isolation from community organizations and practices. Patients pay the price for these artificial barriers, but clinicians do as well. Scattered geographically and few in number, palliative care providers work in relative isolation.
We hoped palliative care practitioners together—as a whole—could have greater impact than individual practitioners working in silos.
To reduce professional isolation and improve continuity across settings, the Delaware Valley Palliative Care Collaborative (DVPCC) was born in 2015—a network of regional palliative care providers. We hoped that the DVPCC could be the vehicle to regularly bring practitioners together, mitigating isolation, and building identity and recognition of the palliative care field. We hoped to use it to foster shared educational and learning opportunities; spread new knowledge and best practices; collaborate with others in the field; strengthen access to palliative care across settings; and have enhanced research opportunities. Palliative care practitioners together—as a whole—could have greater impact than individual practitioners working in silos. And we were right.
Logistics: How it All Came Together
Building a tribe takes persistence and organization; bringing the idea of a palliative care network to reality was accomplished by asking for volunteers from various hospitals and health systems to form a multidisciplinary planning committee of about twelve people. We identified a leader to keep us organized and on track, as it is easy for great ideas to take a back seat to the everyday reality of work and life. The planning committee invited palliative care clinicians in the area to join, requesting that they complete a survey to identify topics of interest for meetings. We also encouraged these providers to forward the invitation to their colleagues, for expanded reach. We settled on meeting as a group four times per year, identified topics and speakers, and asked member hospitals to host our gatherings on a rotation. We also developed a website, as a hub to share ideas and communicate amongst the group.
Impact Thus Far
Before the inception of the DVPCC, palliative care in southeastern Pennsylvania, southern New Jersey, and northern Delaware was silo’d, with virtually no interaction between palliative care providers from different health systems. This included little to no collaboration among the different fellowship programs in the area. Even Fellowship Program Chiefs were relatively unfamiliar with each other and faced many similar problems, seemingly alone.
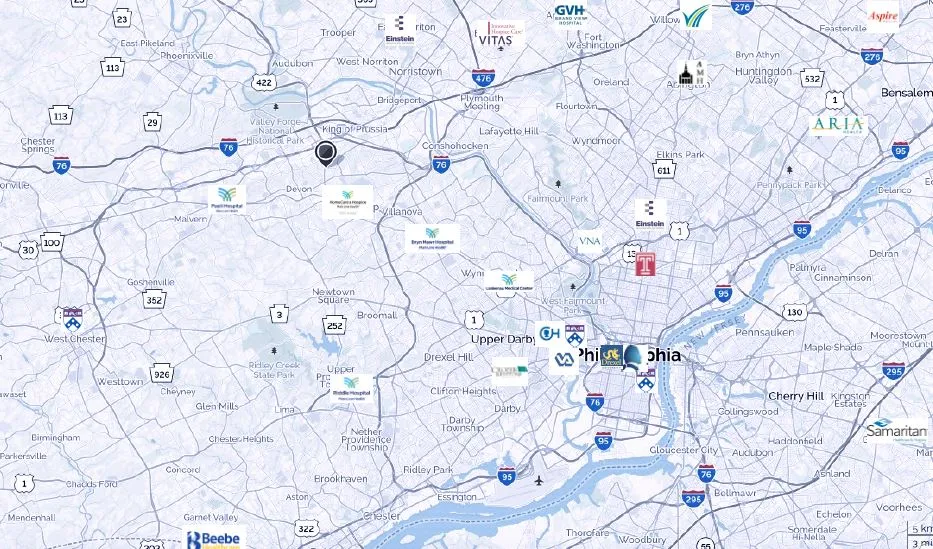
Fifteen clinicians attended the first DVPCC meeting in 2015. Within the first year, we grew to 120 members. At present, our 150 members come from thirty-one hospitals, hospices, and other organizations across the Delaware Valley (see the included map). Attendance at our quarterly meetings ranges from twenty to fifty members; we always make sure to set aside time for networking, which has helped members build important connections.
Our organization has helped the field grow from many local, isolated teams to a much larger regional team, much better able to meet patient and family needs.
Collaboration across the Philadelphia area has increased significantly since forming the DVPCC. Grand Rounds and educational sessions are offered by members from different institutions. Telephone calls are commonly made between palliative care teams when a patient followed by one team transfers to another hospital, even when changing health systems. Providers of outpatient palliative care, still a relatively limited resource in our area, are now known to clinicians, and referrals are often made to ‘competing’ health systems’ palliative care programs to enable care closer to patients’ homes. Many of us at the DVPCC feel that our organization has helped our field grow from many local, isolated teams to a much larger regional team, much better able to meet patient and family needs.
Plans for the Future
The DVPCC has just begun to flourish. This year, a mentoring program will begin; pairs will be established based on self-identified needs, roles, seniority, and training. Some members, for example, have self-identified as mentors for clinical needs, but as mentees for program development or financial sustainability. There is also discussion about offering the DVPCC as a convening venue for our area Hospice and Palliative Medicine (HPM) fellows (six total programs, with ten confirmed fellows for 2018-2019), to create a community for support and peer mentoring.
Additional goals and plans include pursuing non-profit status, which would enable tax-deductible fundraising; the lack of current organizational resources requires the ongoing benevolence of member-institutions to fund meetings. With continued growth and engagement, there’s also potential for the development of a regional intensive palliative care skills course which would help with the onboarding of new clinicians and offer intentional learning and teaching opportunities for HPM fellows. Lastly, we may be able to support an Advanced Practice Provider (APP) fellowship program across settings, including academic and community; inpatient and outpatient; and urban and suburban programs to create a rich, well-rounded experience for learners and to further strengthen interdisciplinary workforce capacity in our region.
Members have found rich collaboration, valuable friendships, and company for what was previously institution-level loneliness and isolation.
The members of the DVPCC have found rich collaboration, valuable friendships, and company for what was previously institution-level loneliness and isolation. We encourage other areas with similar constraints to create a palliative care collaborative, to build your tribe and create a seamless network of palliative care services for our patients and their families.

